Contributors: Barbara Handelin, Ph.D. and Karyn Polak
To learn more about Barbara and Karyn, click here.
![]()
Financialization of the Biomedical System is Failing Us
As we discussed in Part 1 of this article, decades of free-flowing venture capital (VC) funding from the origins of that financial structure in the 20th century – funding that was high-cost for high-risk carrying the potential for high-reward – did deliver great benefits for a period of time, yielding a broad and deep pool of scientific and medical knowledge. Yet that same VC system has since grown to favor almost exclusively those discoveries that are most likely to offer swift and outsized returns, especially those that by their nature throw off a lifetime or extended revenue stream. This narrow focus and incentive structure unfortunately produces products that address less than 10% of all disease conditions, leaving behind the bulk of what is extremely valuable to human beings suffering from disease, but which isn’t valuable by VC standards.
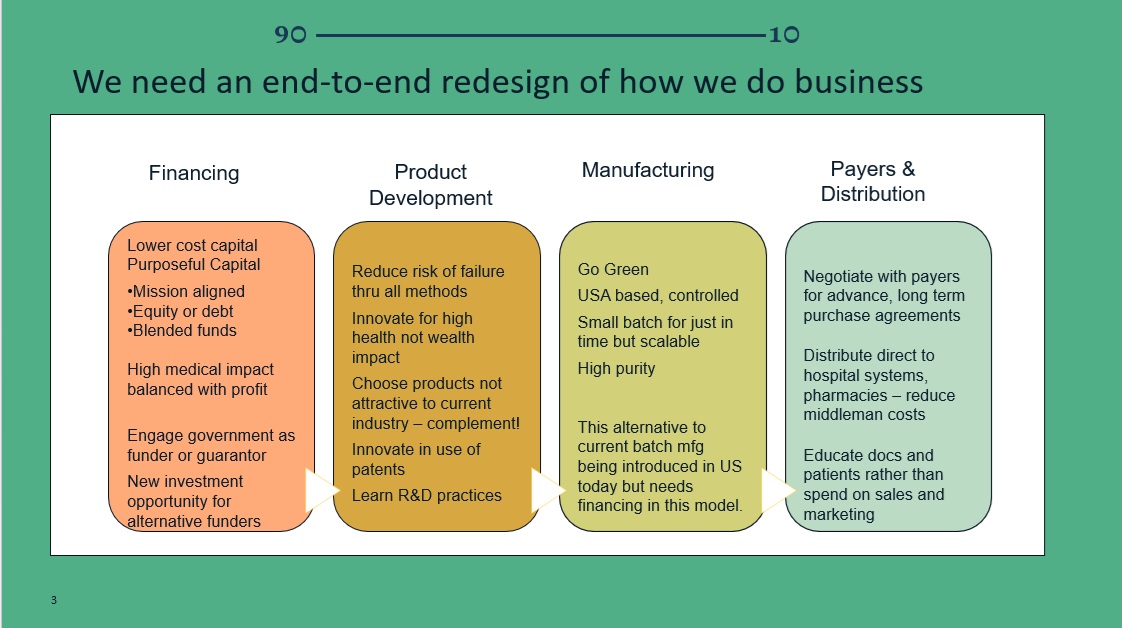
What will it take to change this picture? Intentional Capital: a Biomedical Industry v2.0
Seasoned biotech industry professionals and other accomplished connections including the authors formed a public benefit non-profit entity, The 90~10 Institute, to tackle these medical and economic failures by proposing to stand up a new biomedical industry: Biotech v2.0. Our vision for Biotech v2.0 activates the heart and soul of scientists, philanthropists, and investors to serve the original mission of the biomedical industry: to care for the greatest number of people and treat the greatest number of health challenges possible, in the most efficient way.
Our Theory of Change is that a new biomedical industry (comprised of emerging companies seeking to operate leanly, focused first and foremost on health, thinking outside patent protections, competing on quality and price, and letting profits flow in measure) will produce affordable medicines for the 90%. We believe the entire process can be optimized for maximum productivity and efficiency, producing sustainable profits in a competitive marketplace.1
There are, of course, other levers that must be pulled to advance the work of closing the 90% gap: for example, price controls and other counter pressures on pricing applied by institutional buyers (insurers, health systems, Medicare). The 90~10 Institute recognizes the productive measures being taken by others on these fronts, including federal legislation to allow Medicare/Medicaid to negotiate prices on some (few) treatments, disruptive companies like CostPlusDrugs offering lower prices on novel buying platforms, and non-profit companies like CivicaRx and Medicines 360 providing low-cost drugs to subscribers and to developing world populations at no cost. The 90~10 Institute will support and advocate alongside those efforts, while focusing its energies on educating stakeholders on the pillars depicted above, encouraging aggregation of mission-aligned capital and amplifying the efforts of those willing to put these models into practice.
The 90~10 Financial Innovation Proposal: Biotech Financing v2.0
Companies in v2.0 will be fueled by risk-adjusted, returns-adjusted, “patient” capital. The 90~10 is developing novel financing vehicles to aggregate mission-aligned capital in professionally managed funds, partnerships, and other structures. The Institute will open-source as well as help activate these vehicles.
This new strategy for financing biotech starts with using what some call “regenerative finance” that focuses on people, planet, and purpose. We describe below what mission-aligned investment means and where it comes from, as well as the legal structures needed to center and maintain that mission.
Apply a Regenerative Finance Approach
Regenerative finance sees money as a means, not as an end. Healthcare by necessity requires caring, love, and passion; an intentional caretaking of people and the planet; and a focus on the relationship between provider and patient, indeed on the patient as the purpose first and foremost. That’s why The 90~10 Institute positions regenerative finance as a necessary condition to advance a patient-first biomedical industry.
Apply Mission-Aligned Investment
Sourcing and aggregating investments in Biotech Financing v2.0 to deliver sustainable profit while focusing on maximizing healthcare outcomes could be called purposeful investing, impact investing, or mission-aligned investing.2
The combination of tools needed to serve the mission will depend on the challenges to be addressed. For example, developing drugs from early stages may require “patient” capital; devising one-time-use drugs may require public investments; and facilitating repurposing of existing drugs may require patent policy changes along with mission-aligned capital. Below we describe different types of impact investments that may be needed in one combination or another.3
Philanthropic Capital
When seeking a people-first outcome, often the first type of investment that comes to mind is a grant or philanthropic donation rather than an investment seeking some financial return. Even within the grant structure, though, there are different types that can be brought to bear:
- a straight grant or donation;
- a recoverable grant that under pre-determined circumstances becomes repayable in whole or in part;
- a guarantee that supports the organization’s debts; or
- some combination that catalyzes – encourages or draws in – other investments.
These tools are typically deployed by foundations (public, private, community, or corporate), family offices, public or private endowments, donor-advised funds, or individuals.
On their own, though, grants or philanthropic donations will be insufficient to scale to Biotech Financing v2.0. We propose a change in philanthropy, equity, and debt financing.
Flexible Debt
On the debt side there are a variety of tools, typically involving greater flexibility on the mechanism for a return on the investment:
- a straight term loan, or a more “patient” loan that defers or does not pay interest over a period of time or for the life of the loan;
- revenue- or royalty-based finance that pays interest only upon and as a pre-determined percentage of revenue earned;
- a line of credit that provides a backstop in case it is needed but doesn’t require ongoing interest or principal payments;
- market-based social impact bonds, like Green Bonds; or
- a pay-for-success structure where repayments are made only as and when certain pre-determined, observable social impacts – for example, effectiveness in disease modification or eradication – have been achieved. That flexible approach to return on investment or ROI yields not only a timing benefit but also provides the space to seek sustainable rather than maximum profits.
“Patient” Equity
Equity can be creatively crafted to support a medical purpose-first model of operation. Often a traditional equity investor, e.g., a venture capital or private equity fund, seeks high growth and high returns in a very short period of time and will demand controlling interest through their equity. Controlling the equity position of these investors results in companies focusing on products that, despite long development cycles, can be projected to produce outsized profits if and when they achieve FDA approval for marketing. In the meantime, investors trade on the high scale of future profits, thus satisfying quicker returns than the products can deliver through revenue. Ironically, the need is thus for patient capital seeking modest, reliable returns. This type of investment might involve:
- A SAFE, or Simple Agreement for Future Equity, that provides rights to the investor for a future ownership piece of the enterprise but for which the level of ownership isn’t determined unless and until a specified event occurs.
- A variable dividend vehicle where the shareholders receive distributions (dividends) only if there is available excess cash and then only based upon a previously agreed formula.
- A third, even more patient, model is one in which the investor’s exit is pre-negotiated to occur only upon achievement of a certain level of return to the company and is capped at a certain amount (e.g., 2x or 3x the original investment) - and is often paired with an agreement that the company can buy back the investment rather than it being sold to a third party. The equity might be self-liquidating, such that it is repaid using a pre-determined formula, like available free cash flow up to a specified cap. The equity may even be structured to return to the company for the benefit of its employees.
These patient forms of equity allow maximum likelihood of the enterprise retaining its mission focus rather than losing control to a profit-maximizing outsider.
Multiple Pathways to Mission
Debt and equity tools such as these can be deployed not only by private credit providers (including angel investors, charitable loan funds, diversified business funds) and traditional financial institutions (banks, community development financial institutions (CDFIs), community development companies, credit unions, and faith-based institutions) but also by the very same foundations and endowments that support straight grants, because they can use assets invested to continue their mission even beyond their program-related investments or grants. Patient advocacy organizations (medical research organizations) dedicated to raising funds for diagnostic and therapeutic product development may offer investment support.
Other types of institutions, like investment and social impact funds, research institutions, and others also provide this kind of financing. Healthcare management organizations, healthcare insurance providers, and governmental entities are also players in this market for mission-driven finance.
Even the for-profit corporations that lead the current biomedical industry (v1.0) should be among those willing to step in to help fill the capital gap through more impact-focused financing in order to demonstrate commitment and accountability to public health and to healthcare accessibility, not to mention their patient-first claims.
The more examples and successes demonstrated by the use of these tools, the more likely they will be to spur further innovation and thus the more arrows in the delivery quiver there will be to access. The key to all of these tools is the mission-preservation and independence from the conflicts and pressures that profit-maximization presents. By aligning ownership, governance, and financing with purpose – often called “steward ownership,”4 founders can create a resilient, enduring force field against those common obstacles and advance the development of Biotech Financing v2.0.
Different combinations of the tools we’ve described here will be required for the different types of delivery, access, and affordability challenges in chipping away at that 90% target. In Part 3 of this series, we offer just one blueprint to consider.
Contact Barbara at: [email protected]
Contact Karyn at: [email protected]
References
-
New operating models for product producers is the subject of another paper.
-
The Global Impact Investment Network offers the most widely recognized and consistent resource on impact investing, including a description of its core characteristics.
-
Boston Impact Initiative offers an interactive, user-friendly card deck that provides greater detail on types of capital, potential funding sources, and even transaction structures for impact.
-
Purpose Foundation offers extensive resources and support for steward ownership.